By Lisa Larrimore Ouellette, Nicholson Price, Rachel Sachs, and Jacob Sherkow
Health systems worldwide are facing shortages of crucial medical supplies, including personal protective equipment (PPE), diagnostic testing components including kits and nasal swabs, and even ventilators or ventilator parts. Enter 3D printing. A growing network of hobbyists, small-scale makers, 3D printing firms themselves, and even larger companies with some 3D printing capacity are using the technology to help address ongoing shortages in the COVID-19 response.
What kinds of COVID-19-related products are being 3D printed?
3D printing, also called additive manufacturing, involves building a 3D form from the bottom up by adding one thin layer of material at a time. (Here’s a handy Congressional Research Service overview.) Many materials can be used, including plastic, metal, or resin. The printer is controlled by a computer which prints based on a computer-assisted design (CAD) file. 3D printers have been used for rapid prototyping or by hobbyists for years, but are more recently being used at larger scale.
3D printing is being used to create a host of products potentially relevant to COVID-19. PPE is perhaps the most common example; many people are producing the headbands of protective face shields; some are printing masks. Nasal swabs are also being printed in substantial numbers (the swabby bit at the end is a bristled resin structure, not cotton fibers like you’d find in a Q-Tip), and have been evaluated by, among others, Beth Israel Deaconess Medical Center. Printing has also been used for more complex components of medical devices, such as ventilator valves or splitters so that patients can share a ventilator—or even most of the components of emergency open-source ventilators.
Monday, April 27, 2020
Friday, April 24, 2020
Who’s Afraid of Section 1498?: Government Patent Use as Versatile Policy Tool
Guest post by Christopher Morten & Charles Duan
Chris Morten (@cmorten2) is the Clinical Teaching Fellow and Supervising Attorney in NYU’s Technology Law and Policy Clinic. Charles Duan (@Charles_Duan) is Director of Technology and Innovation Policy at the R Street Institute.
From vaccines to ventilators to diagnostic tests, technology has dominated response strategies to the ongoing COVID-19 pandemic. Where technology leads, patent law and policy follow. Recently, some attention has turned to federal government patent use under 28 U.S.C. § 1498. Jamie Love of KEI has called on the federal government to explore use of section 1498 in its response to COVID-19, to reduce prices, expand supplies, and ensure widespread, equitable access to patented technologies. (We have, too.) There is a long line of scholarship, including Amy Kapczynski and Aaron Kesselheim, Hannah Brennan et al., Dennis Crouch, Daniel Cahoy, and others discussing the relevance of section 1498 in a variety of contexts.
Yet others have encouraged the government to “tread lightly” and described use of section 1498 as a “nuclear option”—potent but dangerous—because it can be used to make massive interventions in the market for patented products—e.g., by issuing compulsory licenses to patents on high-priced brand-name drugs, “breaking” patent monopolies and accelerating the entry of numerous generic competitors. One recent example: a few years ago, Gilead’s high prices on hepatitis C drugs exacerbated a different public health crisis and prompted a chorus of voices, including Senator Bernie Sanders and the New York Times editorial board, to call on the federal government to exercise its section 1498 power to “break” Gilead’s patents in just this way, which might have saved tens of billions of dollars in public spending. (The federal government did not do so.)
Irrespective of the merits of 1498 as a general matter, in the context of a crisis such as the COVID-19 pandemic we see real value in bold, “nuclear option” use of section 1498 to save billions on high-priced prescription drugs and maximize their availability. But that is not the only way section 1498 can be used. It can also be used in modest, incremental, unexceptional ways—it can be as much as a scalpel or a Swiss Army knife as a nuclear weapon, and some of its virtues in this regard have gone underappreciated.
Accordingly, we highlight four particularly valuable features of government patent use under section 1498 in a crisis like the present one: (1) speed, (2) flexibility, (3) ex post determination of the appropriate compensation, and (4) determination of that compensation by an impartial adjudicator. In particular, we compare section 1498 with an alternative policy tool, patent buyouts, which can also expand public access to patented technologies, and identify several reasons why section 1498 may be the preferable tool.
Chris Morten (@cmorten2) is the Clinical Teaching Fellow and Supervising Attorney in NYU’s Technology Law and Policy Clinic. Charles Duan (@Charles_Duan) is Director of Technology and Innovation Policy at the R Street Institute.
From vaccines to ventilators to diagnostic tests, technology has dominated response strategies to the ongoing COVID-19 pandemic. Where technology leads, patent law and policy follow. Recently, some attention has turned to federal government patent use under 28 U.S.C. § 1498. Jamie Love of KEI has called on the federal government to explore use of section 1498 in its response to COVID-19, to reduce prices, expand supplies, and ensure widespread, equitable access to patented technologies. (We have, too.) There is a long line of scholarship, including Amy Kapczynski and Aaron Kesselheim, Hannah Brennan et al., Dennis Crouch, Daniel Cahoy, and others discussing the relevance of section 1498 in a variety of contexts.
Yet others have encouraged the government to “tread lightly” and described use of section 1498 as a “nuclear option”—potent but dangerous—because it can be used to make massive interventions in the market for patented products—e.g., by issuing compulsory licenses to patents on high-priced brand-name drugs, “breaking” patent monopolies and accelerating the entry of numerous generic competitors. One recent example: a few years ago, Gilead’s high prices on hepatitis C drugs exacerbated a different public health crisis and prompted a chorus of voices, including Senator Bernie Sanders and the New York Times editorial board, to call on the federal government to exercise its section 1498 power to “break” Gilead’s patents in just this way, which might have saved tens of billions of dollars in public spending. (The federal government did not do so.)
Irrespective of the merits of 1498 as a general matter, in the context of a crisis such as the COVID-19 pandemic we see real value in bold, “nuclear option” use of section 1498 to save billions on high-priced prescription drugs and maximize their availability. But that is not the only way section 1498 can be used. It can also be used in modest, incremental, unexceptional ways—it can be as much as a scalpel or a Swiss Army knife as a nuclear weapon, and some of its virtues in this regard have gone underappreciated.
Accordingly, we highlight four particularly valuable features of government patent use under section 1498 in a crisis like the present one: (1) speed, (2) flexibility, (3) ex post determination of the appropriate compensation, and (4) determination of that compensation by an impartial adjudicator. In particular, we compare section 1498 with an alternative policy tool, patent buyouts, which can also expand public access to patented technologies, and identify several reasons why section 1498 may be the preferable tool.
Tuesday, April 21, 2020
Regulatory Responses to N95 Respirator Shortages
By Lisa Larrimore Ouellette, Nicholson Price, Rachel Sachs, and Jacob Sherkow
Our recent posts have highlighted shortages in three COVID-19-related knowledge goods: testing, drugs (such as those needed to put patients on ventilators), and clinical trial information about effective treatments. This week we focus on the role of legal regulators in another critical shortage: N95 respirators, one of the key forms of personal protective equipment (PPE) for healthcare workers. We explain how N95 regulation, like COVID-19 testing, presented an interagency coordination problem. The FDA has successfully removed key regulatory hurdles—though the problem should have been anticipated earlier, and much more needs to be done to ensure an adequate supply.
What are N95 respirators?
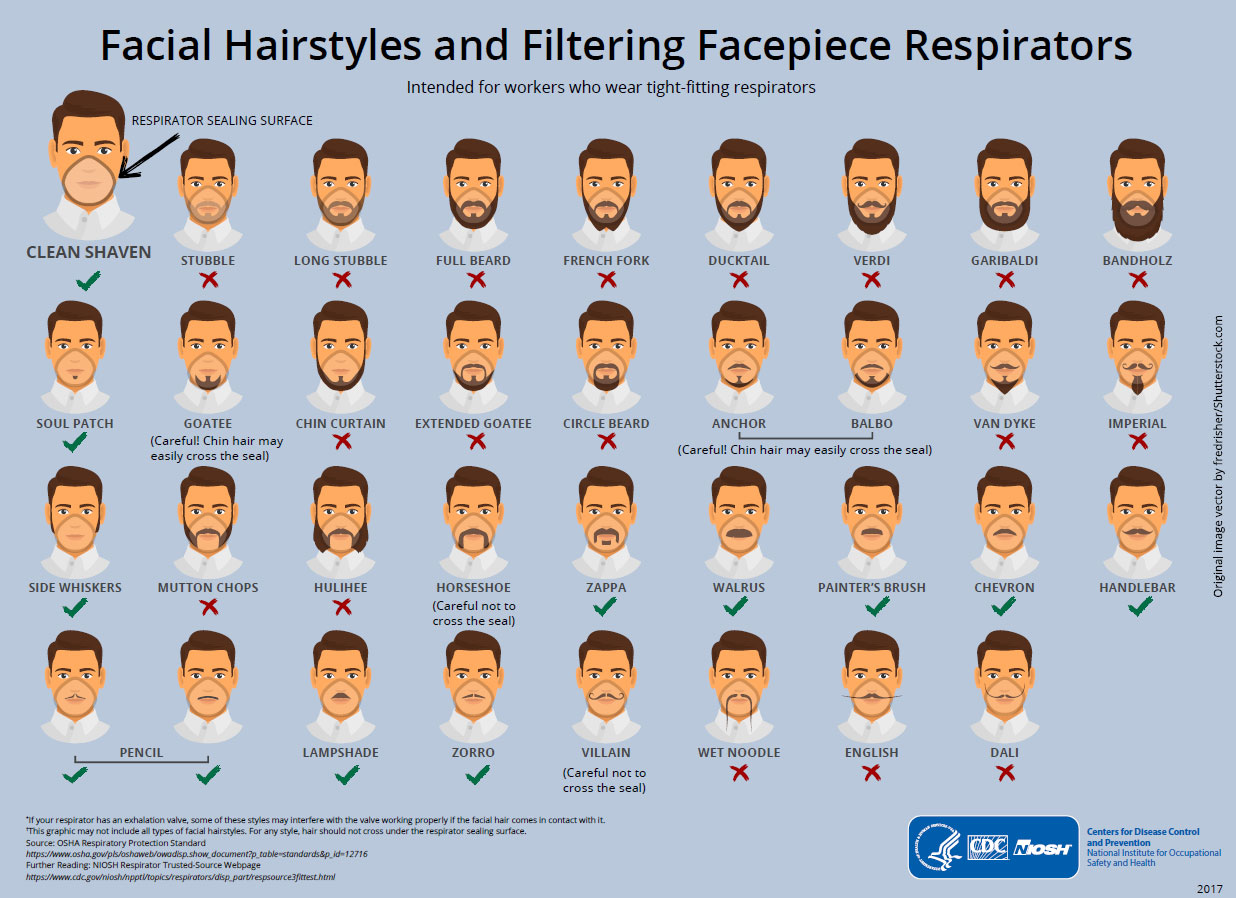
N95 respirators are a specialized subset of face masks (here’s a handy NY Times explainer with photos). A normal surgical mask (what you see, for example, in a typical medical TV show) fits fairly loosely around the face; it blocks splashes and relatively large droplets, but not tiny particles. An N95 respirator, on the other hand, is relatively rigid rather than being flexible, and is designed to fit closely to the face and create a tight seal—tightly enough that the masks don’t work with certain beards (or for children). The “95” in N95 refers to the requirement that the mask block at least 95% of 0.3 micron particles (about a thousandth the width of a human hair). Both types of masks are meant to be single-use.
N95 masks are meant to keep droplets that include the SARS-CoV-2 virus out. They’re not perfect, but if they’re well fitted, they are effective at protecting the wearer (most crucially right now, the healthcare providers who are caring for patients and are themselves still getting sick in droves). Surgical masks, on the other hand, do a worse job of keeping the virus out. Cloth masks even less so. But cloth masks can help keep droplets in—that is, if someone is sick, wearing a cloth mask may keep them from projecting droplets that can infect other people. The CDC now recommends that everyone wear a face mask when in public, to avoid infecting other people (because even asymptomatic individuals can infect others, and the lack of testing means it’s very hard for most people to know whether they have been infected). However, surgical masks and especially N95 masks are in very short supply, and should be reserved for medical professionals.
N95s were initially developed for industrial uses including mining. The key feature—and what makes N95s harder to manufacture than other masks—is that the masks are made using what’s called “melt-blown” fabric. A polymer (such as polystyrene, polyurethane, or nylon), is melted then blown through small nozzles; it forms a matrix of tiny fibers with many holes (think: cotton candy), which can capture particles. But the machines to make this fabric are complex and expensive, and manufacturers of the fabric are struggling—and failing—to meet demand.
Our recent posts have highlighted shortages in three COVID-19-related knowledge goods: testing, drugs (such as those needed to put patients on ventilators), and clinical trial information about effective treatments. This week we focus on the role of legal regulators in another critical shortage: N95 respirators, one of the key forms of personal protective equipment (PPE) for healthcare workers. We explain how N95 regulation, like COVID-19 testing, presented an interagency coordination problem. The FDA has successfully removed key regulatory hurdles—though the problem should have been anticipated earlier, and much more needs to be done to ensure an adequate supply.
What are N95 respirators?
N95 respirators are a specialized subset of face masks (here’s a handy NY Times explainer with photos). A normal surgical mask (what you see, for example, in a typical medical TV show) fits fairly loosely around the face; it blocks splashes and relatively large droplets, but not tiny particles. An N95 respirator, on the other hand, is relatively rigid rather than being flexible, and is designed to fit closely to the face and create a tight seal—tightly enough that the masks don’t work with certain beards (or for children). The “95” in N95 refers to the requirement that the mask block at least 95% of 0.3 micron particles (about a thousandth the width of a human hair). Both types of masks are meant to be single-use.
{kind=link}
N95 masks are meant to keep droplets that include the SARS-CoV-2 virus out. They’re not perfect, but if they’re well fitted, they are effective at protecting the wearer (most crucially right now, the healthcare providers who are caring for patients and are themselves still getting sick in droves). Surgical masks, on the other hand, do a worse job of keeping the virus out. Cloth masks even less so. But cloth masks can help keep droplets in—that is, if someone is sick, wearing a cloth mask may keep them from projecting droplets that can infect other people. The CDC now recommends that everyone wear a face mask when in public, to avoid infecting other people (because even asymptomatic individuals can infect others, and the lack of testing means it’s very hard for most people to know whether they have been infected). However, surgical masks and especially N95 masks are in very short supply, and should be reserved for medical professionals.
N95s were initially developed for industrial uses including mining. The key feature—and what makes N95s harder to manufacture than other masks—is that the masks are made using what’s called “melt-blown” fabric. A polymer (such as polystyrene, polyurethane, or nylon), is melted then blown through small nozzles; it forms a matrix of tiny fibers with many holes (think: cotton candy), which can capture particles. But the machines to make this fabric are complex and expensive, and manufacturers of the fabric are struggling—and failing—to meet demand.
Wednesday, April 15, 2020
How can innovation and regulatory policy accomplish robust COVID-19 testing?
By Lisa Larrimore Ouellette, Nicholson Price, Rachel Sachs, and Jacob Sherkow
It’s now clear that expansive, population-wide testing is part-and-parcel of every successful COVID-19 containment strategy. But US testing efforts, from the beginning of the pandemic until now, have been widely criticized as lacking. Perhaps as a direct consequence of this failure, the US now leads the world in COVID-19 cases and deaths. What are these tests and what’s our capacity to test; why is it important to test; how have the FDA and other administrative agencies addressed the issue; and what can we do about it?
What is the status of US testing capacity?
It is important to distinguish between two types of COVID-19 tests: reverse transcription polymerase chain reaction (RT-PCR) tests for SARS-CoV-2, the virus that causes COVID-19; and serological tests for the body’s immune response to SARS-CoV-2. The tests are not interchangeable: RT-PCR tests detect the presence of the virus’s genome, itself, and thus determine whether someone is currently infected. Someone who was once infected and has since recovered will return a negative result. A serological test, by contrast, detects whether the body has produced antibodies to the virus; that’s useful to determine whether someone has been infected for long enough to mount an immune response.
To date, virtually all of the testing has been of the RT-PCR type, useful for answering the question: Is the patient infected now? Testing centers in the US are currently running approximately 135,000 tests a day—far fewer per capita than in other countries. The US’s maximum, overall testing capacity is unclear and is, in any event, a moving target given that new tests are now being cleared by the FDA with some frequency. But it’s widely acknowledged that testing is not at the level that it needs to be to accurately assess the number of people infected with SARS-CoV-2.
There are myriad reasons for this deficit in testing: an initially slow ramp-up of tests approved by the FDA; difficulties in speeding manufacturing of kits used to conduct the tests; a shortage of reagents to conduct the tests, including solutions, primers, and even the swabs used to collect samples from patients; the capacity of clinical laboratories to run tests and return results; and less technical hang-ups like patients’ difficulties in finding or physical getting to testing sites and questions concerning who will pay for such testing.
It’s now clear that expansive, population-wide testing is part-and-parcel of every successful COVID-19 containment strategy. But US testing efforts, from the beginning of the pandemic until now, have been widely criticized as lacking. Perhaps as a direct consequence of this failure, the US now leads the world in COVID-19 cases and deaths. What are these tests and what’s our capacity to test; why is it important to test; how have the FDA and other administrative agencies addressed the issue; and what can we do about it?
What is the status of US testing capacity?
It is important to distinguish between two types of COVID-19 tests: reverse transcription polymerase chain reaction (RT-PCR) tests for SARS-CoV-2, the virus that causes COVID-19; and serological tests for the body’s immune response to SARS-CoV-2. The tests are not interchangeable: RT-PCR tests detect the presence of the virus’s genome, itself, and thus determine whether someone is currently infected. Someone who was once infected and has since recovered will return a negative result. A serological test, by contrast, detects whether the body has produced antibodies to the virus; that’s useful to determine whether someone has been infected for long enough to mount an immune response.
To date, virtually all of the testing has been of the RT-PCR type, useful for answering the question: Is the patient infected now? Testing centers in the US are currently running approximately 135,000 tests a day—far fewer per capita than in other countries. The US’s maximum, overall testing capacity is unclear and is, in any event, a moving target given that new tests are now being cleared by the FDA with some frequency. But it’s widely acknowledged that testing is not at the level that it needs to be to accurately assess the number of people infected with SARS-CoV-2.
There are myriad reasons for this deficit in testing: an initially slow ramp-up of tests approved by the FDA; difficulties in speeding manufacturing of kits used to conduct the tests; a shortage of reagents to conduct the tests, including solutions, primers, and even the swabs used to collect samples from patients; the capacity of clinical laboratories to run tests and return results; and less technical hang-ups like patients’ difficulties in finding or physical getting to testing sites and questions concerning who will pay for such testing.
Tuesday, April 7, 2020
How can the US address coronavirus drug shortages?
By Lisa Larrimore Ouellette, Nicholson Price, Rachel Sachs, and Jacob Sherkow
The escalating pandemic has caused devastating shortages not only of ventilators and personal protective equipment like masks, but also of essential medicines needed to treat COVID-19 patients. As detailed by STAT and the New York Times, prescriptions for painkillers, sedatives, anesthetics, and antibiotics are up, but the rate at which prescriptions are filled and shipped to hospitals is down. The FDA helpfully tracks drug shortages, but this doesn’t solve the problem. With the sudden spike in hospitalized patients with COVID-19 symptoms, physicians are using these drugs faster than manufacturers are making them.
What is causing these drug shortages?
Drug shortages are frighteningly common even in the best of times. A 2019 FDA report noted that from 2013 to 2017, at least 163 drugs went into shortage. (The actual number is likely much higher.) That report blamed “economic forces”—namely, price-eroding generic competition, a lack of incentives to make quality generic manufacturing more efficient, and supply chain difficulties that made the continued manufacture of older generics unprofitable. These problems are now exacerbated by the sudden demand spikes caused by COVID-19 patients. As just one example: propofol, an important drug for sedating patients who need intubation—and, historically, already in waxing and waning states of shortage—has seen prescriptions shoot up about 100%.
Supply has been slow to meet COVID-19-related demand—but slower still because of the outbreak’s disruption to the global supply chain. Many pharmaceutical ingredients are manufactured in China, which has seen slowdowns (and in some cases, shutdowns) in manufacturing sectors across the country. Furthermore, because drugs do expire, they’re not stockpiled when there’s a surplus. In some instances, countries have banned the export of drug products important for treating COVID-19 to ensure adequate supply for their own citizens. India, for example, has banned exports on hydroxychloroquine in the event the drug proves useful in treating COVID-19. It’s a wicked problem: the very thing causing the sudden spike in demand is shutting down the means of supply.
The escalating pandemic has caused devastating shortages not only of ventilators and personal protective equipment like masks, but also of essential medicines needed to treat COVID-19 patients. As detailed by STAT and the New York Times, prescriptions for painkillers, sedatives, anesthetics, and antibiotics are up, but the rate at which prescriptions are filled and shipped to hospitals is down. The FDA helpfully tracks drug shortages, but this doesn’t solve the problem. With the sudden spike in hospitalized patients with COVID-19 symptoms, physicians are using these drugs faster than manufacturers are making them.
What is causing these drug shortages?
Drug shortages are frighteningly common even in the best of times. A 2019 FDA report noted that from 2013 to 2017, at least 163 drugs went into shortage. (The actual number is likely much higher.) That report blamed “economic forces”—namely, price-eroding generic competition, a lack of incentives to make quality generic manufacturing more efficient, and supply chain difficulties that made the continued manufacture of older generics unprofitable. These problems are now exacerbated by the sudden demand spikes caused by COVID-19 patients. As just one example: propofol, an important drug for sedating patients who need intubation—and, historically, already in waxing and waning states of shortage—has seen prescriptions shoot up about 100%.
Supply has been slow to meet COVID-19-related demand—but slower still because of the outbreak’s disruption to the global supply chain. Many pharmaceutical ingredients are manufactured in China, which has seen slowdowns (and in some cases, shutdowns) in manufacturing sectors across the country. Furthermore, because drugs do expire, they’re not stockpiled when there’s a surplus. In some instances, countries have banned the export of drug products important for treating COVID-19 to ensure adequate supply for their own citizens. India, for example, has banned exports on hydroxychloroquine in the event the drug proves useful in treating COVID-19. It’s a wicked problem: the very thing causing the sudden spike in demand is shutting down the means of supply.
Subscribe to:
Posts (Atom)