By Lisa Larrimore Ouellette, Nicholson Price, Rachel Sachs, and Jacob Sherkow
Our recent posts have highlighted shortages in three COVID-19-related knowledge goods: testing, drugs (such as those needed to put patients on ventilators), and clinical trial information about effective treatments. This week we focus on the role of legal regulators in another critical shortage: N95 respirators, one of the key forms of personal protective equipment (PPE) for healthcare workers. We explain how N95 regulation, like COVID-19 testing, presented an interagency coordination problem. The FDA has successfully removed key regulatory hurdles—though the problem should have been anticipated earlier, and much more needs to be done to ensure an adequate supply.
What are N95 respirators?
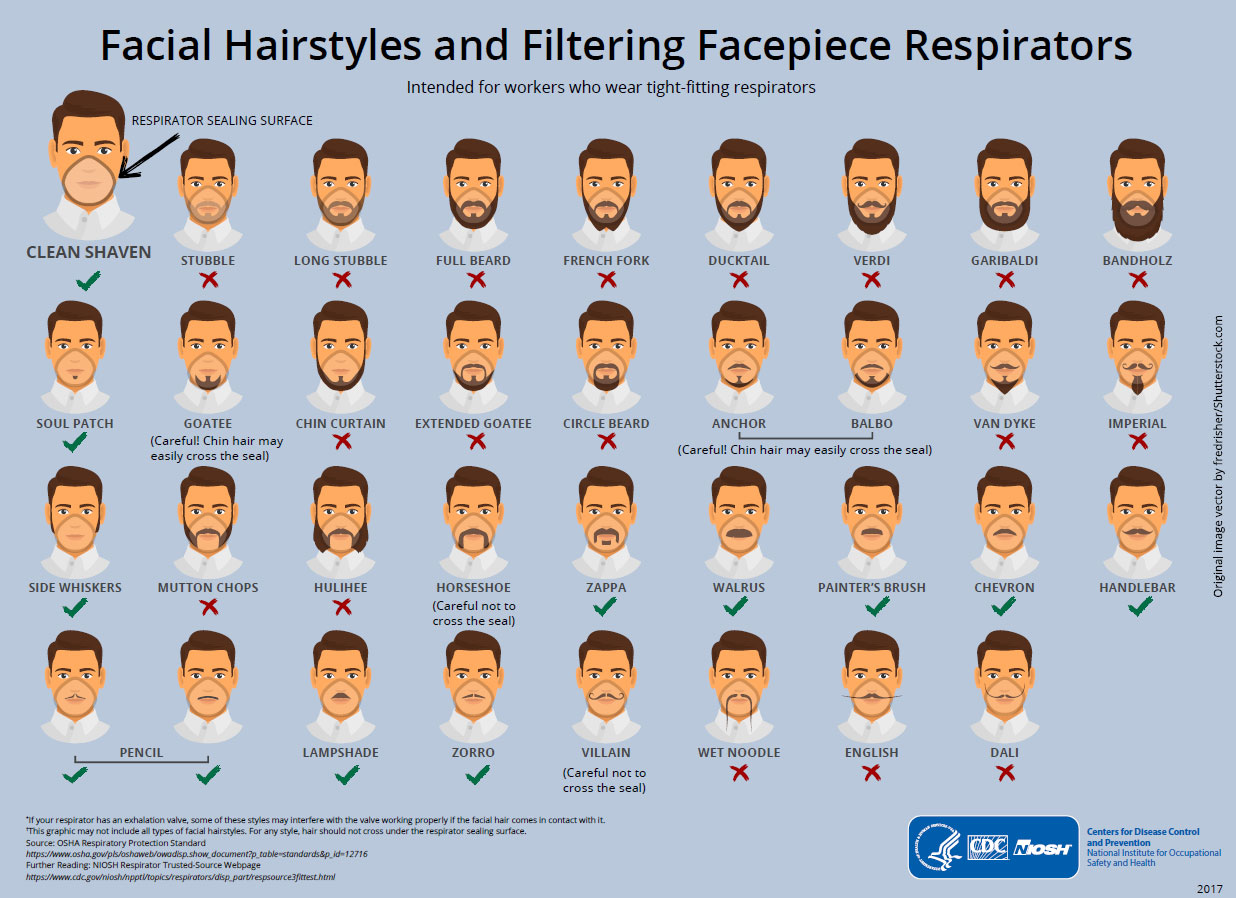
N95 respirators are a specialized subset of face masks (here’s a handy NY Times explainer with photos). A normal surgical mask (what you see, for example, in a typical medical TV show) fits fairly loosely around the face; it blocks splashes and relatively large droplets, but not tiny particles. An N95 respirator, on the other hand, is relatively rigid rather than being flexible, and is designed to fit closely to the face and create a tight seal—tightly enough that the masks don’t work with certain beards (or for children). The “95” in N95 refers to the requirement that the mask block at least 95% of 0.3 micron particles (about a thousandth the width of a human hair). Both types of masks are meant to be single-use.
N95 masks are meant to keep droplets that include the SARS-CoV-2 virus out. They’re not perfect, but if they’re well fitted, they are effective at protecting the wearer (most crucially right now, the healthcare providers who are caring for patients and are themselves still getting sick in droves). Surgical masks, on the other hand, do a worse job of keeping the virus out. Cloth masks even less so. But cloth masks can help keep droplets in—that is, if someone is sick, wearing a cloth mask may keep them from projecting droplets that can infect other people. The CDC now recommends that everyone wear a face mask when in public, to avoid infecting other people (because even asymptomatic individuals can infect others, and the lack of testing means it’s very hard for most people to know whether they have been infected). However, surgical masks and especially N95 masks are in very short supply, and should be reserved for medical professionals.
N95s were initially developed for industrial uses including mining. The key feature—and what makes N95s harder to manufacture than other masks—is that the masks are made using what’s called “melt-blown” fabric. A polymer (such as polystyrene, polyurethane, or nylon), is melted then blown through small nozzles; it forms a matrix of tiny fibers with many holes (think: cotton candy), which can capture particles. But the machines to make this fabric are complex and expensive, and manufacturers of the fabric are struggling—and failing—to meet demand.
Who regulates N95s?
N95s’ origin as industrial respirators helps explain the strange double regulation of the respirators. They’re principally regulated by the National Personal Protective Technology Laboratory, which is part of the National Institute for Occupational Safety and Health (NIOSH), which is part of the CDC. (As a side note, it’s interesting that although NIOSH is a National Institute studying health, it’s not part of the National Institutes of Health, and although it does research on occupational safety and health, it’s not part of the Occupational Safety and Health Administration. Such are the vagaries of federal bureaucracy.) However, while NIOSH regulates all N95 respirators, those intended for use in medical settings are also regulated by the FDA as medical devices. The two agencies started coordinating more closely on this in 2018 with a Memorandum of Understanding (MOU) between the agencies so that normal N95s used in construction and industrial jobs are evaluated by NIOSH and exempt from the FDA’s 510(k) premarket clearance process, and N95s for healthcare settings (including ones for a particular disease, or with antimicrobial function) go through 510(k).
All of this, of course, is domestic; N95 masks are regulated around the globe by different regulators in different countries, which set slightly different standards. 3M has a helpful comparison chart. Given that the basic product is the same, it is unfortunate in retrospect that the slightly different standards have led to a more fragmented supply chain; without regulatory action, for instance, N95 masks approved for use in South Korea were not automatically approved for use in the United States. Regulators, however, have been acting to reduce these barriers.
How have N95 regulators responded to COVID-19?
Regulating medical devices requires tradeoffs between risk and access. If regulation is too lax, users will face unwarranted safety risks. If regulation is too strict, access will be delayed and limited. In normal times, careful scrutiny of N95 masks may make sense to protect healthcare workers. But when the CDC suggests healthcare workers use bandanas and doctors are pleading for masks on social media, it is worth relaxing regulations that pose access barriers—particularly ones that reflect different policy choices by other countries without a strong evidence base to support one standard over another.
As we explained last week, to circumvent normal review processes during a public health emergency, the FDA can use Emergency Use Authorizations (EUAs), which it has done repeatedly to address PPE shortages caused by the pandemic. On March 2, the FDA granted the CDC's EUA request to allow healthcare personnel to use NIOSH-approved respirators—i.e., respirators typically used in construction and similar industrial jobs. On March 24, the agency issued another EUA allowing importation of non-NIOSH-approved respirators from Australia, Brazil, Europe, Japan, Korea, and Mexico. China’s KN95 respirators were excluded from this list due to concerns about “inauthentic product,” but on April 3, the FDA added them to the list.
The FDA can also lower regulatory burdens by exercising “enforcement discretion,” or choosing not to enforce certain regulations. The agency published an enforcement policy for respirators on March 25 and revised the policy April 2 indicating that it “does not intend to object to the distribution and use of face masks” that do not comply with specified regulatory requirements “where the face mask does not create an undue risk in light of the public health emergency.” The FDA and the CDC have also provided more general guidance on addressing the shortage.
In some ways, this is a story of regulators successfully removing barriers to access—but it is also a story of regulatory catch-up to a problem that shouldn’t have taken policymakers by surprise. By the end of January, N95s were out of stock in consumer stores, clinics were running low, and an Atlantic story titled “We Don’t Have Enough Masks” outlined the problem. Decreasing the fragmentation of N95 supply chains could have happened much sooner.
Who pays for N95s?
Removing the above-described regulatory hurdles can help lower the costs of companies seeking to bring more N95 masks to market. But companies can also be encouraged to increase the availability of N95 masks by the presence of a strong demand signal for the products. Yet payment for N95s (and PPE in general) is typically not directly charged to individual patients and their insurers, in ways that might attenuate the demand signal for PPE relative to those for drugs or devices (which can be billed for directly).
Typically, pre-COVID-19, hospitals or other organizations acting on behalf of providers would purchase PPE for use in their facilities, and that PPE would usually not be directly reimbursed. It would be factored into other hospital charges and not billed separately, at least for most major insurance programs. (There are a few exceptions here—for instance, for those insurers who still pay hospitals a percent of their charges, those hospitals can bill for PPE off of their chargemaster. Critical access hospitals are reimbursed on the basis of their costs, which might therefore include PPE as well.)
Now, amid the pandemic, many hospital systems continue to attempt to purchase their own PPE, but many states or cities are also seeking to centralize orders on behalf of their providers. This type of governmental involvement has a number of advantages. In the context of N95 shortages, as we currently observe, centralizing purchasing at the city or state level may enable purchasing entities to obtain better prices for these scarce products by purchasing larger quantities. Perhaps more importantly, these governmental entities are often able to access federal funds to support their purchase of PPE, having declared particular types of authorized emergencies due to the pandemic.
One problem with current efforts to procure PPE of all kinds, including N95 respirators, is the seemingly contradictory positions of the federal government. Trump Administration officials have frequently said that states must be in charge of their own acquisition of PPE, and attempted to deflect responsibility for a nationally coordinated strategy on that front. On its own, this has resulted in bidding wars between the states for PPE, which drives prices up even further (some of which the federal government then pays, as noted above). However, the federal government itself has often come in and either purchased PPE from under the states or has confiscated purchases from state governments. The federal government even seems to be interfering in health systems’ efforts to acquire PPE, as the chief physician executive of a health system in Massachusetts recently chronicled in the New England Journal of Medicine. These responses have further exacerbated the difficulties providers have in obtaining adequate PPE for their staff.
What other steps can policymakers take to address N95 shortages?
Broadly speaking, policymakers have three options to address the N95 shortage: make more masks; make better use of existing masks; and import masks.
Like procuring critical materials during wartime, the most robust authority for producing more N95s is the oft-discussed, much-confused Defense Production Act. Title I of the DPA, if invoked, would allow the President to order businesses to prioritize manufacturing N95s over other equipment. (There’s also Title III, which would allow the administration to offer loans and guarantees for private businesses to purchase respirators, although it’s unclear how that would immediately solve the manufacturing shortage.) Getting clearer numbers on the number of masks needed relative to what’s out there would enable the President to set manufacturing targets across a broad set of manufacturers without crippling their production of other important goods. Whether the President needs to formally invoke the DPA—or just threaten to do so—is unclear; there have been many manufacturers who have volunteered to retool their manufacturing plans to make masks. Nonetheless, it’s doubtful such volunteerism is enough to meet the overwhelming and ongoing demand for respirators.
Centralized coordination of production has another salutary benefit: it could also be used to smooth allocation of the masks among states, helping them avoid bidding wars and defensive stockpiling. In the absence of such coordination, states have been prey to price gouging from private vendors, selective sales, and even lawsuits. State attorneys general have responded in kind but—again—such skirmishes could be avoided with more centralized coordination of manufacturing.
Aside from making new masks, policy makers could focus on better ways to reuse old ones. In ideal circumstances, protective masks, including N95s, should not be reused, for obvious reasons. But today’s circumstances are leagues away from ideal and efforts to find acceptable ways to reuse masks have included attempts at sterilization. Recently posted studies, for example, have suggested that masks can be decontaminated several times with vaporized hydrogen peroxide or UV light. In an odd way, this reuse is a form of innovation itself and sanctioned, in at least one instance by, FDA.
These manufacturing and reusing bottlenecks suggest that U.S. policymakers should also consider importing more N95s from abroad, especially as coronavirus outbreaks begin to subside in some countries. This would align with the impetus behind previous free trade agreements enacted in prior administrations; the coronavirus pandemic demonstrates the benefits of well-functioning global supply markets. True: some of the difficulties in importing N95s today are regulatory; as noted, N95s are not tested to the same specifications in the U.S. as elsewhere. But differences seem quite slight, especially given the crisis and the supply shortage: does a max pressure drop inhalation resistance of 343 vs. 350 pascals mean that much in a time of crisis? Policymakers interested in getting the U.S. back to work should get back to basics: manufacturing and reusing what we have and importing the rest.
{kind=link}